Case Study
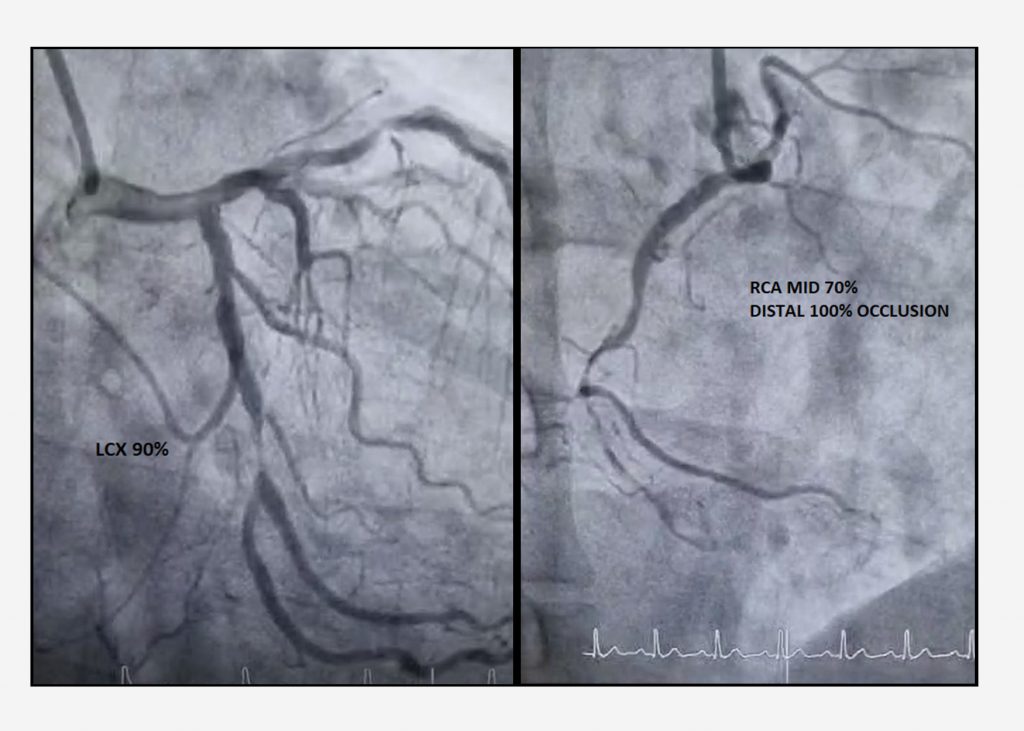
Coronary Artery Bypass Grafting Surgery on a Young Male with Strong Family History of CAD
Coronary Artery Disease or CAD is labeled “premature,” before age 55 years for men or 65 years for women.
Coronary Artery Disease or CAD is labeled “premature,” before age 55 years for men or 65 years for women.